Before the novel coronavirus (COVID-19), telehealth adoption in ambulatory care was inconsistent.1 Now, many clinicians have been dumped in at the telehealth deep end—and it’s sink or swim.2,3 Without the ability to provide healthcare for payment, primary-care clinicians unable to offer video visits are vulnerable to financial collapse.4–7 And in the post-pandemic future, those without video visits will likely remain vulnerable, as telehealth has become an essential modality of care.8 In the words of Seema Verma, “I think the genie’s out of the bottle on this one.”9
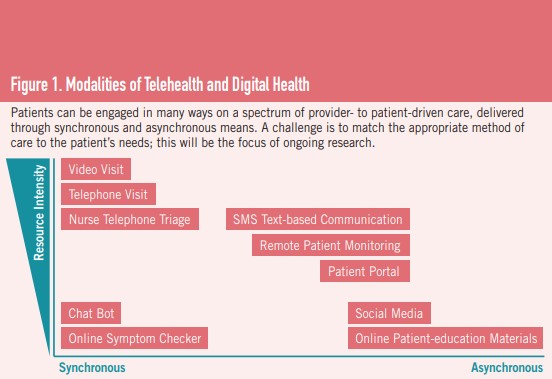
Here, we outline seven steps for successful telehealth adoption, drawn from our experience transforming nine primary-care practices (see Figure 1).
1. Prepare yourself
Understand your feelings, thoughts, and knowledge gaps; educate yourself; and acquire the skills necessary for success. While in-person care is the gold standard, it is neither appropriate or necessary in all situations in order to provide safe and effective high-quality care.
2. Prepare patients—see the digital divide
Telehealth is new to most patients, and some research suggests that increased adoption will exacerbate health inequities.10–14 Overall, one in four Americans may not have digital-literacy skills or access to internet-enabled digital devices to engage in telemedicine visits.15 Factors that disadvantage certain populations can be addressed with education and training for patients, and by connecting patients to free or reduced-cost broadband services through governmental digital-inclusion response efforts.16,17 It is also important to offer phone visits as an alternative and ensure that interpreter services are available.
Another digital-inclusion strategy is to reach out to patients to prepare them for telemedicine visits. We utilize a “virtual visit concierge” model, which initiates multiple outreach attempts before each visit to help prepare patients.
3. Acquire the appropriate tools and technology
There are many platforms available for video visits. When selecting one, consider reliability, ease of use, stability on all types of devices (smartphone, tablets, and laptop/desktop computers), and responsiveness of the vendor to technical-support inquiries. Complement video visits with other digital-health strategies. Telephone visits and nurse telephone triage are other forms of synchronous patient communication. We also utilize patient portals and text-based encounters to allow asynchronous communication and expand access. Remote patient-monitoring tools can further expand the scope of care; see Figure 1.
4. Prepare your team
Revised workflows can prepare you for successful telemedicine visits. We created workflows and scripting for all teams; it is important to map the standard work for scheduling, patient preparation, patient check-in, and follow-up around video visits.
Recognize that your team may have their own barriers to technology adoption, and consider appointing a digital health navigator to be a resource for patients and staff. The navigator should be available to patients and providers for consultations and problem-solving, to help implement patient-outreach strategies, to participate in quality-improvement efforts, and to monitor metrics such as equity in access, patient experience, and provider experience.
5. Have a good visit
Clinical decision-making and establishing rapport are foundational to a good healthcare visit. Clinical decision-making through telemedicine care is limited by the inability to conduct a physical exam, but there are workarounds and new opportunities available. Physical distancing need not result in social distance or the disruption of continuity of care, a fundamental tenet of primary care.18, 19
To inform clinical decision-making, use telehealth services to obtain patient-reported vitals, conduct a patient-directed exam (e.g., direct the patient to palpate their own abdomen), augment the exam with peripherals (e.g., tele-stethoscope information), obtain data from wearable monitors, direct the patient to adjust camera angles to better visualize pathologies,
and/or have a friend or family member present at the visit (a.k.a. a “tele-presenter”) to assist with any of the above. Patient-reported vitals in particular are valid for clinical decision-making and are accepted for Medicare Wellness Visits.20
Incorporate the new opportunities to enhance care that telehealth makes possible. Look at a patient’s collection of medications, assess their living situation, interview friends and family who may not normally attend visits, and follow up frequently.
Techniques for building rapport are transferrable to video visits and are likely already a part of your practice.21 Briefly, these techniques include preparing with intention, listening intently and completely, agreeing on what matters most, connecting with the patient’s story, and exploring emotional cues. Skills specific to video visits include making eye contact by looking at the camera and selecting appropriate lighting, backgrounds, and settings to ensure visual clarity and patient privacy.
6. Assess outcomes and adapt
Consider convening a team with representation from front-desk staff, medical assistants, back-office staff, patients, and providers to assess professional, organizational, and quality metrics such as provider satisfaction, productivity, throughput time, staff effort level, and completion of healthcare-maintenance activities like depression screenings. We created a digital health dashboard to drive our improvement work in this regard.
7. Advocate for payment reform
During the COVID-19 pandemic, payers have improved reimbursement for telemedicine. However, enhanced payments for telehealth services are set to expire. If rates return to pre-pandemic levels, a significant roadblock to adoption, maintenance, and sustainability will reemerge. Loss of payment for telephone encounters would be particularly detrimental to patients who do not own a computer or smartphone, have unreliable internet access, and/or are uncomfortable with technology. Even if enhanced payments for telehealth are extended, further reform is required. In the absence of comprehensive payment reform, payment rates should be higher for medical homes than for immediate-care or telemedicine-only sites of care, since the former offer robust chronic-disease management, whereas immediate-care or telehealth-only practices provide a narrower scope of care.
Indeed, meaningful payment reform would enable the flexible delivery of care and more freedom to serve patients. Comprehensive payment for primary care would allow a focus on quality of care and enable the deployment of transformational telehealth—not just a temporary substitution for office visits.
CONCLUSION
During the COVID-19 pandemic, many ambulatory practices have quickly adopted telehealth to continue care while mitigating the risk of transmission.22,23 Telehealth is a potentially transformative model of healthcare delivery; but like any new technology, it comes with benefits and challenges. The steps laid out above offer an approach to help implement these services and/or improve the way in which they are provided.
Advocacy for continued payment for telehealth is needed, as is research about the quality of and satisfaction with telehealth care. Finally, and perhaps most importantly, this work must be done in a way that improves access for patients caught on the other side of the digital divide. We must take advantage of this opportunity to re-envision primary care through a more equitable lens.
Indeed, meaningful payment reform would enable the flexible delivery of care and more freedom to serve patients. Comprehensive payment for primary care would allow a focus on quality of care and enable the deployment of transformational telehealth—not just a temporary substitution for office visits.
References
1 Chokshi, D.A. “The Health Innovation We Need.” JAMA, 2018;320(5):427-429; doi:10.1001/jama.2018.9545
2 CDC. “Adjusting the Way Healthcare Services Are Delivered During the COVID-19 Pandemic.” Coronavirus Disease 19 Healthcare Facility Guidance, U.S. Department of Health & Human Services. June 11, 2020. https://bit.ly/3lvWT0Z
3 Hollander, J.E. and Carr, B.G. “Virtually Perfect? Telemedicine for COVID-19.” N Engl J Med, 2020; 382:1679-1681 DOI: 10.1056/NEJMp2003539.
4 Patient-Centered Primary Care Collaborative. “Clinician Survey.” Quick COVID-19 Primary Care Survey, The Larry A. Green Center. March 13, 2020. https://bit.ly/34L686y
5 Kimball, S. “Doctors Face Pay Cuts, Furloughs and Supply Shortages As Coronavirus Pushes Primary
Care to the Brink.” Health and Science, CNBC LLC. May 25, 2020. https://cnb.cx/2GSS6HI
6 Terry, K. “Primary Care Practices Struggle to Survive Despite Visit Rebound.” Medscape Medical News, WebMD LLC. May 22, 2020. https://wb.md/2GSSfuK
7 Westfall, J.M, Stange, K., DeVoe, J., Jaen, C., Bazemore, A., Hester, C., Cohen, D., and Phillips, R. “Coronavirus: Family Physicians Provide Telehealth Care at Risk of Bankruptcy.” Opinion, USA Today, Gannett Satellite Information Network, LLC. April 7, 2020. https://bit.ly/3iMWZzB
8 Mehrotra, A., Chernew, M., Linetsky, D., Hatch, H., and Cutler, D. “The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges.” COVID-19, The Commonwealth Fund. https://bit.ly/33K2eeS
9 Dyrda, L. “’The Genie’s Out of the Bottle on This One’: Seema Verma Hints at the Future of Telehealth for CMS Beneficiaries.” Telehealth, Becker’s Hospital Review, Becker’s Healthcare. https://bit.ly/3dflrZ6
10Wallace, L.S., Angier, H., Huguet, N., Gaudino, J.A., Krist, A., Dearing, A.M., Killerby, M., Marino, M., and DeVoe, J.E. “Patterns of Electronic Portal Use among Vulnerable Patients in a Nationwide Practice-based Research Network: From the OCHIN Practice-based Research Network (PBRN).” The Journal of the American Board of Family Medicine. 2016, 29(5):592-603; DOI: https://bit.ly/34JbeQO
11 Arcaya, M.C. and Figueroa, J.F. “Emerging Trends Could Exacerbate Health Inequities in the United States.” Health Affairs. 2017, 36 (6):992-998;doi:10.1377/hlthaff.2017.0011.
12 Lyles, C., Schillinger, D., and Sarkar, U. “Connecting the Dots: Health Information Technology Expansion and Health Disparities.” PLoS Med. 2015, 12(7): e1001852. doi:10.1371/ journal.pmed.1001852.
13Perrin, A. “Digital Gap between Rural and Nonrural America Persists.” Factank News in the Numbers, Pew Research Center. https://pewrsr.ch/30Sl1Db
14Khoong, E.C., Rivadeneira, N.A., Hiatt, R.A., and Sarkar, U. “The Use of Technology for Communicating with Clinicians or Seeking Health Information in a Multilingual Urban Cohort: CrossSectional Survey.” J Med Internet Res 2020; 22(4):e16951; doi:10.2196/16951.
15Nouri, S., Khoong, E.C., Lyles, C.R., and Karliner, L. “Addressing Equity in Telemedicine for Chronic Disease Management During COVID-19 Pandemic.” NEJM Catalyst 2020; doi: 10.1056/CAT.20.0123.
16Pew Research Center. Internet/Broadband Fact Sheet. Internet and Technology, Pew Research Center. June 12, 2019. https://pewrsr.ch/3jLkFW9
17NDIA. State Government COVID-19 Digital Inclusion Response, COVID-19 Resources, National
Digital Inclusion Alliance. June 12, 2020. https://bit.ly/3nAgvmA
18Bergman, D., Bethell, C., Gombojav, N., Hassink, S., and Stange, K.C. “Physical Distancing with Social Connectedness.” Annals of Family Medicine, 2020, 18(3):272-277; doi:10.1370/afm.2538.
19Cheng, A., Vasquez-Guzman, C.E., Duffield, T., and Hofkamp, H. “Advancing the 5 C’s & Health Equity with Telemedicine in Family Medicine.” Telemedicine and E-Health. (Published online, ahead of print.) July 28, 2020.
20FPM Editors. “How to Collect Patient Vitals for Telehealth Visits, Including AWVs.” Practice Pearls, Family Practice Management, American Academy of Family Physicians. May 20, 2020. https://bit.ly/317hXTV
21Zulman, D.M., Haverfield, M.C., Shaw, J.G., et al. “Practices to Foster Physician Presence and Connection with Patients in the Clinical Encounter.” JAMA, 2020;323(1):71-81; doi:10.1001/jama.2019.19003.
22Devoe, J.E., Cheng, A., and Krist, A. “Regional Strategies for Academic Health Centers to Support Primary Care During the COVID-19 Pandemic: A Plea from the Front Lines.” JAMA Health Forum, American Medical Association. April 8, 2020. https://bit.ly/34A3DUw
23Krist, A.H., DeVoe, J.E., Cheng, A., and Ehrlich, T. “The Five Phases of Pandemic Care for Primary Care”. Annals of Family Medicine, COVID-19 Collection. (Preprint.) https://bit.ly/3iKUcH7